
Patent Foramen Ovale (PFO)
Introduction
The foramen ovale is a small hole located in the septum, the wall between the two upper chambers of the heart. Before birth, the lungs are not used to get blood rich in oxygen. Instead, this blood comes from the mother’s placenta and is delivered through the umbilical cord. The foramen ovale makes it possible for the blood to go directly from the veins to the right atrium of the fetus’ heart to the left atrium of the heart, bypassing the lungs. Normally, the foramen ovale closes as blood pressure rises in the left side of the heart after birth, or within a few years after birth. Once it is closed, the overall blood flows to the lungs without bypass, to get oxygen before it enters the left side of the heart and gets pumped to the rest of the body.
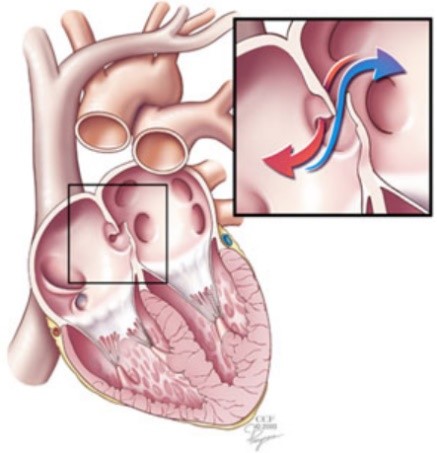
The foramen ovale remains open, or patent (patent foramen ovale or PFO), in about 25% of the adult population [1] (1). Most patients with a PFO do not have any symptoms. However, the condition may play a role in migraine headaches and it increases the risk of stroke, transient ischemic attack and heart attack. In divers, it has been associated with severe neurological decompression sickness, inner ear decompression sickness, and cutaneous symptoms [2]. Venous bubbles formed during and after decompression can pass through the foramen ovale shunt -so not filtered by the lung- and invade the peripheral arterial circulation. They can reach tissues supersaturated with inert gases and, as a result, there is an amplified risk of bubble emboli in these zones.
Literature overview
The correlation between the presence of a PFO and an increased risk of occurrence of a serious form of decompression sickness was mentioned more than thirty years ago [3], in particular concerning neurological forms which develop rapidly after the return to the surface [4].
The various forms of DCS for which a link has been demonstrated regarding the presence of PFO have been recently reviewed [2]. Cerebral DCS seem more linked to PFO presence than spinal cord DCS [5]. The correlation to the risk of spinal cord DCS is less marked but seems to exist [6] [7]. Regarding brain and inner ear injuries, where supersaturation levels can be locally high, mechanisms have been proposed and discussed [2] [8]. The relationship between cutaneous forms and PFO was initially more puzzling. A recent study leads to hypothesize a cerebrally mediated mechanism [9].
The DCS risk ratio for diver with PFO compared to diver without PFO is not precisely known but several studies tend to point a two 2.5 times risk increase at least [10] [11] and even more than five [12] [13]. Severe DCS forms are definitely more frequent when a PFO is present [14]. Additionally, the size of the PFO appears to play a major role regarding DCS risk ratio determination [12][15]. In a recent study, on the 200 divers who had an atrial defect closure (PFO and ASD) following shunt-related DCS, about 50% had an atrial defect 10mm or larger, whereas about 1% of the general population appear to have PFO diameter in this range (about 25% of the population have a PFO but with a diameter mainly between 2mm and 6mm) [15]. Nevertheless, serious DCS forms are sometimes associated with small size PFO [16].
PFO closure appears to be an efficient solution to strongly limit the passage of bubbles towards the arterial aspect [17] and to prevent major DCS and return to unrestrictive diving [16][18], while conservative diving profiles without PFO closure seems also to lead to satisfying level of safety regarding severe DCS forms [18]. It is also associated with a decrease of asymptomatic brain lesions [19]. PFO closure surgery is characterized by a low rate of procedural complication [20].
Discussion
DCS risk characterization linked to a PFO presence remains a major research topic. A rigorous statistical analysis is not yet available. A routine way of screening PFO (presence, dimension, fully, partially, intermittently opened…), with or without a DCS case history, with or without invasive means, is not feasible or even advisable.
Indeed, whereas the scientific community agrees on the fact that PFO is a DCS risk factor, a routine screening of diver is not preconized [20]. Only divers with an history of severe DCS form are eligible for a routine screening, through bubble contrast transthoracic echocardiography with provocative manoeuvres. In case of positive PFO result, PFO close using transcatheter is recommended for return to normal diving [21].
However, a conservative approach of diving, with less severe diving profiles leading to gas load limitation, appears to be an interesting alternative to limit DCS risk [22].
Finally, it must be noticed that other right-to-left shunt pathways may exist in the body, in particular at pulmonary level [23][24], the impact of oxygen and the level of effort on this type of shunt having been studied [24] [25] [26]. Currently, the DCS risk associated with this anatomical reality (with a dispersion of its importance among the population) and its role in microbubble arterialization is poorly known.
References
- Homa S, Messé SR, Rundek T, Sun YP, Franke J, Davidson K, Sievert H, Sacco RL, Di Tullio MR. Patent foramen ovale. Nat Rev Dis Primers. 2016; 2: 15086. – ABSTRACT
- Wilmshurst PT. The role of persistent foramen ovale and other shunts in decompression illness. Diving Hyperb Med. 2015; 45(2):98-104. – FULL TEXT
- Moon RE, Camporesi EM, Kisslo JA. Patent foramen ovale and decompression sickness in divers. Lancet. 1989 Mar 11, 1(8637):513-514. – ABSTRACT
- Wilmshurst PT, Byrne JC, Webb-Peploe MM. Relation between interatrial shunts and decompression sickness in divers. Lancet. 1989 Dec 2, 2(8675):1302-1306. – ABSTRACT
- Germonpré P, Dendale P, Unger P, Balestra C. Patent foramen ovale and decompression sickness in sports divers. Journal of Applied Physiology. 84(5): 1622-1626. – FULL TEXT
- Wilmshurst PT, Bryson P. Relationship between the clinical features of neurological decompression illness and its causes. Clinical Science. 2000; 99:67-75. – FULL TEXT
- Wilmshurst PT. Clinical experience of right-to-left shunts in divers with decompression illness. Patent Foramen Ovale and Fitness to Dive Consensus Workshop, Montreal June 17 2015. pp. 21-33. – FULL TEXT
- Mitchell SJ, Doolette DJ. Pathophysiology of inner ear decompression sickness: potential role of the persistent foramen ovale. Diving Hyperb Med. 2015; 45(2): 105-110. – FULL TEXT
- Kemper TCPM, Rienks R, Van Ooij PJAM, Van Hulst RA. Cutis marmarota in decompression illness may cerebrally mediated: a novel hypothesis on the aetiogoloy of cutis marmarota. Diving Hyperb Med. 2015; 45(2):84-88. – FULL TEXT
- Bove AA. Risk of decompression sickness with patent foramen ovale. Undersea and Hyperbaric Medicine. 1998; 25(3): 175-178. – ABSTRACT
- Germonpre P. Incidence of DCS in divers with RLS – A prospective study. Patent Foramen Ovale and Fitness to Dive Consensus Workshop, Montreal, June 17 2015. pp. 47-58. – FULL TEXT
- Torti SR, Billinger M, Schwerzmann M, Vogel R, Zbinden R, Windecker S, Seiler C. Risk of decompression illness among 230 divers in relation to the presence and size of patent foramen ovale. Eur Heart J. 2004; 25: 1014-1020. – FULL TEXT
- Honek J, Sramek M, Sefc L, Januska J, Fiedler J, Horvath M, Tomak A, Novotny S, Honek T, Veselka J. High-grade patent foramen ovale is a risk factor of unprovoked decompression sickness in recreational divers. J Cardiol. 2019; 74(6): 519-523. –ABSTRACT
- Liou K, Wolfers D, Turner R, Bennett M, Allan R, Jepson N, Cranney G. Patent foramen ovale influences the presentation of decompression illness in SCUBA divers. Heart, Lung and Circ. 2015; 24: 26-31. – FULL TEXT
- Wilmshurst PT, Morrison WL, Walsh KP, Pearson MJ, Nightingale S. Comparison of the size of persistent foramen ovale and atrial septal defects in divers with shunt-related decompression illness and in the general population. Diving Hyperb Med. 2015; 45(2):89-93. – FULL TEXT
- Wilson C, Sayer MDJ. Cerebral arterial gas embolism in a professional diver with a persistent foramen ovale. Diving Hyperb Med. 2015; 45(2): 124-126. – FULL TEXT
- Honek J, Smarek M, Sefc L, Januska J, Fielder J, Horvath M, Tomek A, Novotny S, Honek T, Veselka J. Effect of catheter-based patent foramen ovale closure on the occurrence of arterial bubbles in scuba divers. Journal of The American College of Cardiology Intervention. 2014; 7(4): 403-408. – FULL TEXT
- Koopsen R, Stella PR, Thijs KM, Rienks R. Persistent foramen ovale closure in divers with a history of decompression sickness. Neth Heart J. 2018; 26: 535-539. – FULL TEXT
- Billinger M, Zbinden R, Mordasini R, Windecker S, Schwerzmann M, Meier B, Seiler C. Patent foramen ovale closure in recreational divers: effect on decompression illness and ischaemic brain lesions during long-term follow-up. 2011; 97(23): 1932-1937. – ABSTRACT
- Pearman A, Bugeja L, Nelson M, Szantho GV, Turner M. An audit of persistent foramen ovale closure in 105 divers. Diving Hyperb Med. 2015; 45(2): 94-97. – FULL TEXT
- Smart D, Mitchell S, Wilmshurst P, Turner M, Banham N. Joint position statement on persistent foramen ovale (PFO) and diving. South Pacific Underwater Medicine Society (SPUMS) and the United Kingdom Sports Diving Medical Committee. Diving Hyperb Med. 2015; 45(2): 129-131. – FULL TEXT
- Klingmann C, Rathmann N, Hausmann D, Bruckner T, Kern R. Lower risk of decompression sickness after recommendation of conservative decompression practices in divers with and without vascular right-to-left shunt. Diving Hyperb Med. 2012; 42(3): 146-150. – FULL TEXT
- Lovering AT, Stickland MK, Kelso AJ, Eldridge MW. Direct demonstration of 25 and 50µm arteriovenous pathways in healthy human and baboon lungs. Am J Physiol Heart Circ Physiol. 2007; 292: H1777-H1781. – FULL TEXT
- Lovering AT, Haverkamp HC, Romer LM, Hokanson JS, Eldridge MW. Transpulmonary passage of 99mTc macroaggregated albumin n healthy humans at rest and during maximal exercise. Journal of Applied Physiology. 2009; 106: 1986-1992. – FULL TEXT
- Lovering AT, Romer LM, Haverkamp HC, Pegelow DF, Hokanson JS, Eldridge MW. Intrapulmonary shunting and pulmonary gas exchange during normoxic and hypoxic exercise in healthy humans. Journal of Applied Physiology. 2008; 104: 1418-1425. – FULL TEXT
- Eldridge MW. Inducible intrapulmonary arteriovenous shunt pathways: are they important in DCS?. Patent Foramen Ovale and Fitness to Dive Consensus Workshop, Montreal, June 17 2015. pp. 65-72. – FULL TEXT
(1) In fact, there are two kinds of such holes in the heart. One is called an atrial septal defect (ASD), and the other is a patent foramen ovale (PFO). Although both are holes in the wall of tissue (septum) between the left and right upper chambers of the heart (atria), their causes are quite different. An ASD is a failure of the septal tissue to form between the atria, and as such it is considered a congenital heart defect, something that you are born with. Generally an ASD hole is larger than that of a PFO.